




Prepared for Anette
⏱ Avg. Reading Time: 5 min
More than 1.8 million people in England have diagnosed Chronic Kidney Disease (CKD) and there are an estimated 1.2 million people who have the condition but are undiagnosed.
This leads to increased risk of cardiovascular disease events (e.g. heart failure) and progression to end stage renal disease (ESRD).
Improved identification and treatment of people with CVD is a key pillar of the NHS Long Term Plan, which aims to reduce the incidence of heart attacks, strokes and dementia by improving the quality of care for at-risk patients, including those living with hypertension and diabetes.
According to the most recent National Diabetes Audit, in {{company}} there are currently 45,005 patients with either Type 1 or Type 2 diabetes, 18,300 (41%) of which have not undergone an ACR test in the past year.
It is important to recognise that whilst the COVID-19 pandemic reduced testing rates, performance on this care metric has been historically low.
Especially in comparison with GFR test completion, and this was true even when ACR testing was a requirement of the Quality Outcomes Framework (QOF).
What is already a worrying statistic is magnified when looking at the number of untested patients with the other risk factors highlighted by NICE guidance, such as hypertension and cardiovascular disease.
According to the latest QOF data (2021), there are 77,478 patients in {{company}} with hypertension and best estimates are that only 30% of these will have completed an ACR test, leaving 54,235 people with the potential for undiagnosed CKD.
As outlined above, the risk factors for CKD include diabetes, hypertension, cardiovascular disease and a number of other conditions.
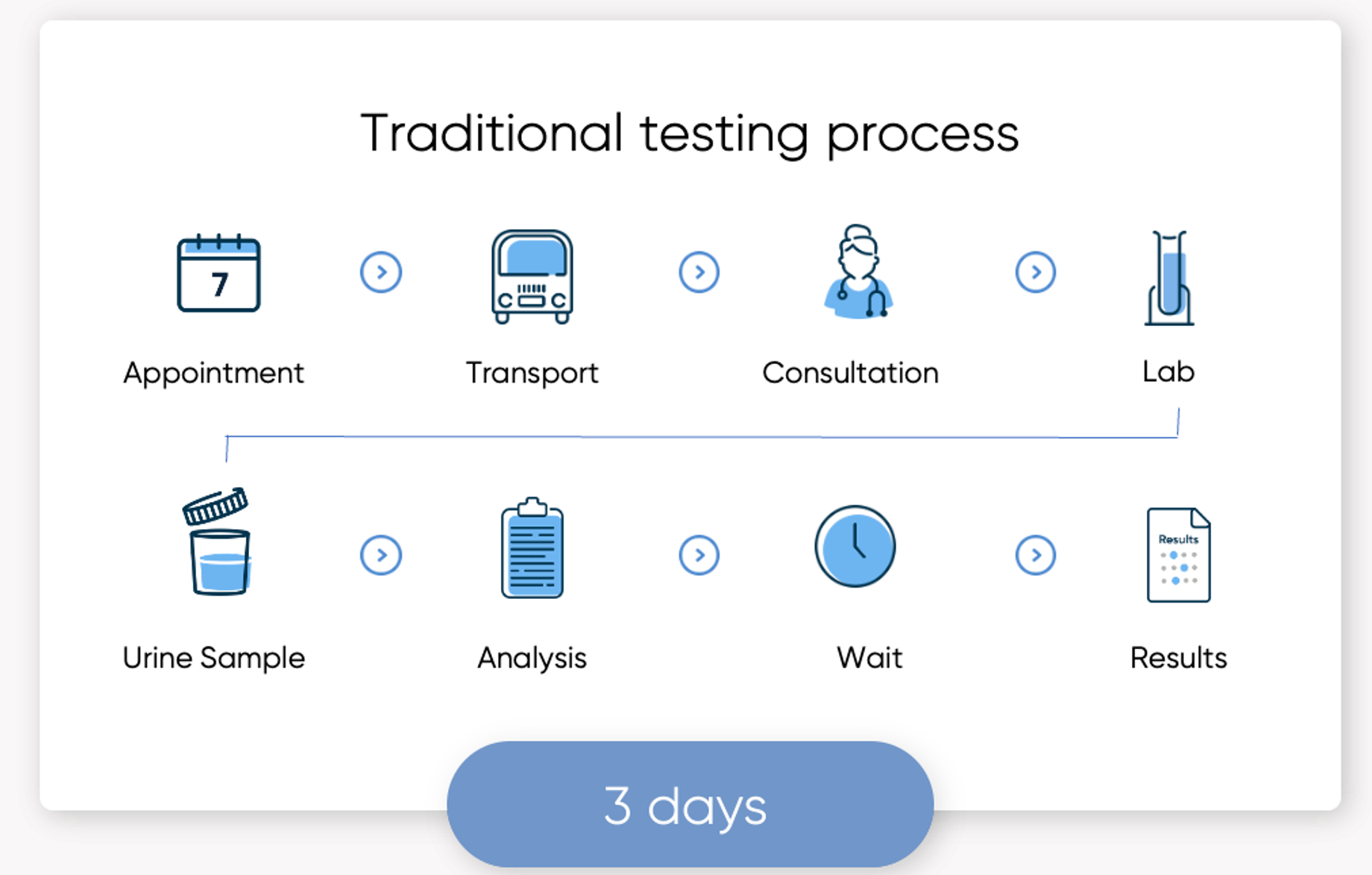
NICE recommends that these patients receive regular tests to check for signs of kidney damage; classification of CKD requires a combination of glomerular filtration rate (GFR, a blood test) and albumin:creatinine ratio (ACR, a urine test).
Although many people with risk factors for CKD receive regular blood tests, test completion rates for ACR are poor.
Analysis of National Diabetes Audit data also demonstrates a six-percentage point gap in uptake of ACR testing between people living in the top and bottom Index of Multiple Deprivation (IMD) deciles.
This indicates that the most deprived communities are even less likely to complete their annual ACR test than the least deprived communities.
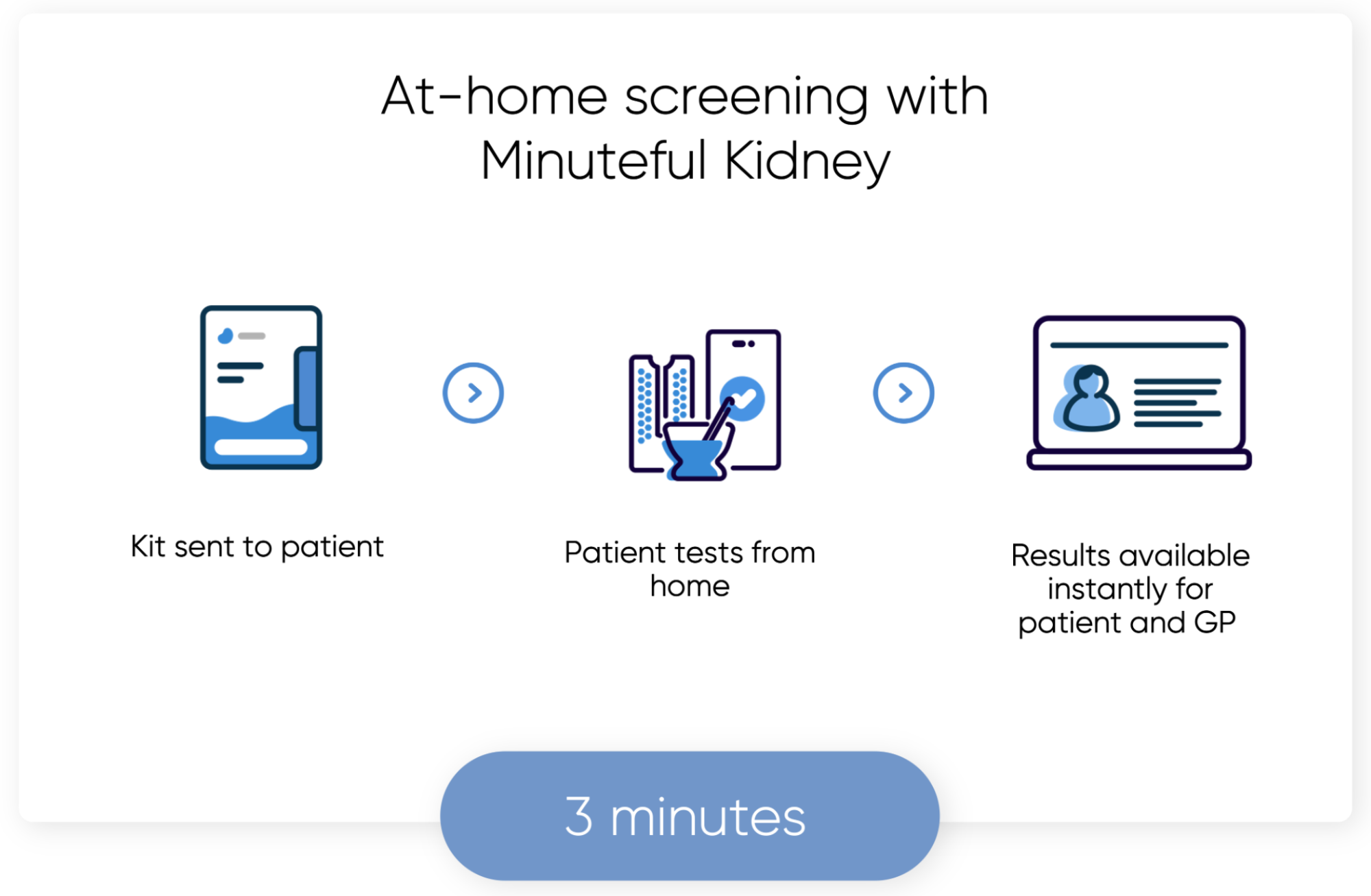
Minuteful Kidney helps narrow the gap and improve uptake with a test that can be performed by the patient at home, with the same level of accuracy as a point-of-care analyser (in a study by Clalit, comparing the performance of Minuteful Kidney against Olympus AU 5800 by Beckman Coulter).
Using colorimetric analysis, computer vision, and AI we transform the smartphone camera into a clinical-grade medical device.
The test is sent to the patient’s home, and a smartphone app walks the user through a simple test, making it as easy as taking a photo.
Results are made immediately available to the patient along with education about next steps and in the electronic patient record for their GP to review.
Frimley ICB has pockets of inequality and 2.3% of the population live in the most deprived region of England.
CKD does not affect everyone equally and is an important area of focus for reducing health inequalities, hence its inclusion in the national CVDPrevent audit.
People from lower socio-economic groups are more likely to develop CKD and progress faster towards kidney failure.
Black, Asian and minority ethnic communities are five times more likely to develop CKD than other groups [3].
Frimley ICB has pockets of inequality and 2.3% of the population live in the most deprived region of England.
CKD does not affect everyone equally and is an important area of focus for reducing health inequalities, hence its inclusion in the national CVDPrevent audit.
People from lower socio-economic groups are more likely to develop CKD and progress faster towards kidney failure.
Black, Asian and minority ethnic communities are five times more likely to develop CKD than other groups [3].
Segmentation of National Diabetes Audit data demonstrates that the ACR testing gap between people in IMD deciles 1-2 (representing 28.6% of the population) and IMD deciles 3-10 declined by 74% in all practices where Minuteful Kidney was introduced, while it stayed effectively unchanged in practices that did not use Minuteful Kidney.
• GP practice sends initial SMS or letter
• Healthy.io send SMS to say kit is on it’s way
• Test kit arrives at patient’s home
• Leaflet provided with test kit
• Initial outreach sequence (if test not completed)
• Patient reminders via text, push notification, email
• Support via call centre
• Patient conducts test
• Results available immediately for GP review and follow-up








